Case report
This case supports the importance of proper pre-operative endodontic evaluation of teeth adjacent to edentulous sites receiving dental implants. This 21-year-old female presented with pain and localized swelling in teeth #6-8 area. The patient had an implant placed in site #7 by another dentist about a year before visiting us. She reported that the endodontic treatment on tooth #6 was completed sometime after the implant placement. The examination showed swelling over the #6-7 area with tenderness to palpation. No purulence noted.
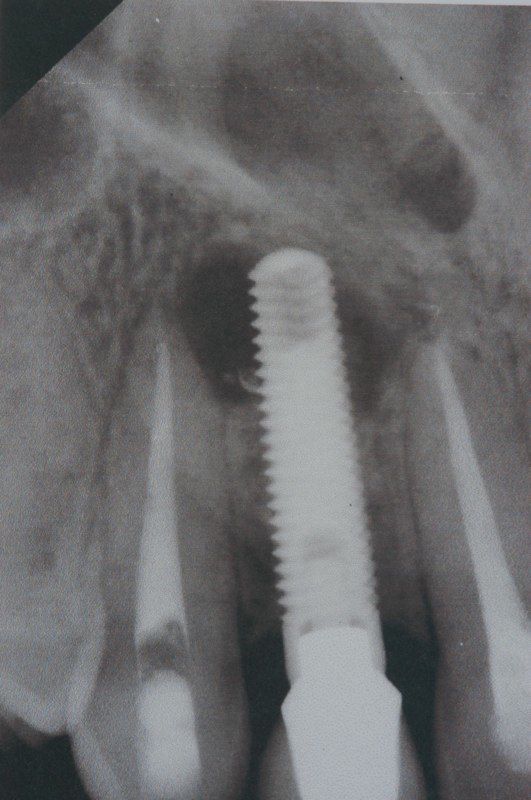
The Periapical X-ray showed a large radiolucent lesion at the apex of the implant extending to tooth #6 (canine); however, there appeared to be bone present between the lesion and apex of tooth #8. The differential diagnosis was periapical cyst or granuloma; however, the origin of the lesion was unknown. Based on history and presentation, tooth #6 was thought to be the origin of this lesion. The implant was stable with no mobility and restored with proper occlusion.
Treatment
Initially, the patient was referred to an endodontist to evaluate tooth #6, which was retreated. The lesion was confirmed to be associated with tooth #6, most likely from an accessory canal or inadequate seal from the initial treatment. Next, a surgical exploration was done by Dr. Kazemi to evaluate the extent of the lesion and its proximity to the implant. The patient was informed that the implant may be compromised significantly and may require removal. A local flap was raised, and the lesion was explored.
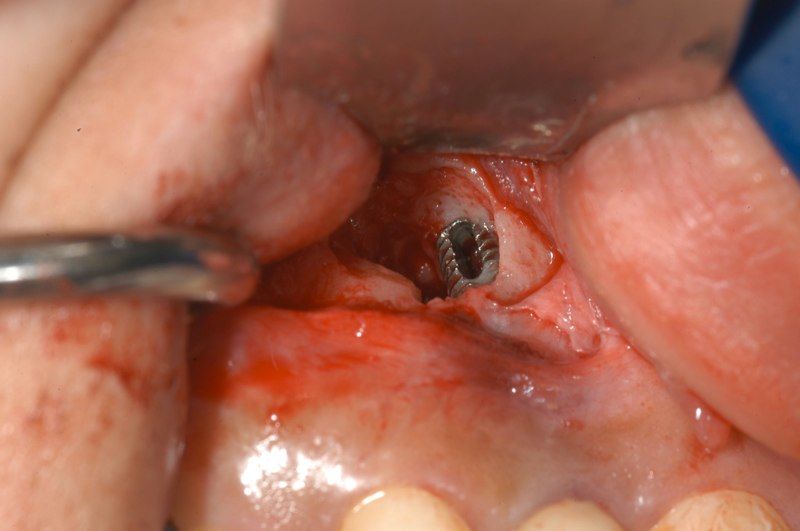
The granulation tissue was excised, and the lesion was noted to involve apical one-third of the implant on the distal, lingual, and facial aspect. The inflammatory tissues were carefully removed, and the site was carefully degranulated. The surface of the implant was treated with tetracycline and gel foam. The site was grafted and covered with GTR membrane.
The patient was followed for about 6 months, and the lesion was noted to heal with the good bony architecture around the implant. Although this was ultimately successful, it is worth noting that contaminated implant surfaces from infection do not predictably heal after such treatment.
Conclusions
- Teeth adjacent to proposed implant sites should always be endodontically evaluated before implant placement. Any teeth with existing RCT or large restorations, or apical pathology, should be evaluated and treated first.
- A CBCT (CT scan) can be highly beneficial in the diagnosis of lesions that can be easily missed on routine dental X-rays.
- The treatment of infected implants with bone grafting is not very predictable and should only be tried in selected cases. The decision should be based on the location of the lesion, the degree of bone defect, amount of implant surface exposure, and characteristics of the implant surface.
Photos




