 Radiographs are an important and necessary part of diagnostics for all patients receiving dental treatment. They reveal dental diseases such as caries, periodontal disease, infections, and trauma as well as various types of pathology and a wide range of dental conditions. They are also critical for planning any type of dental treatment including restorative, teeth extractions, dental implants, root canal treatments, orthodontics, and periodontal therapy.
Radiographs are an important and necessary part of diagnostics for all patients receiving dental treatment. They reveal dental diseases such as caries, periodontal disease, infections, and trauma as well as various types of pathology and a wide range of dental conditions. They are also critical for planning any type of dental treatment including restorative, teeth extractions, dental implants, root canal treatments, orthodontics, and periodontal therapy.
So, what type of X-rays should a dental patient have? Periapical X-rays? A full mouth series? Panorex? Bitewings? CBCT (Cone Beam CT Scan)? In what combination, and how often?
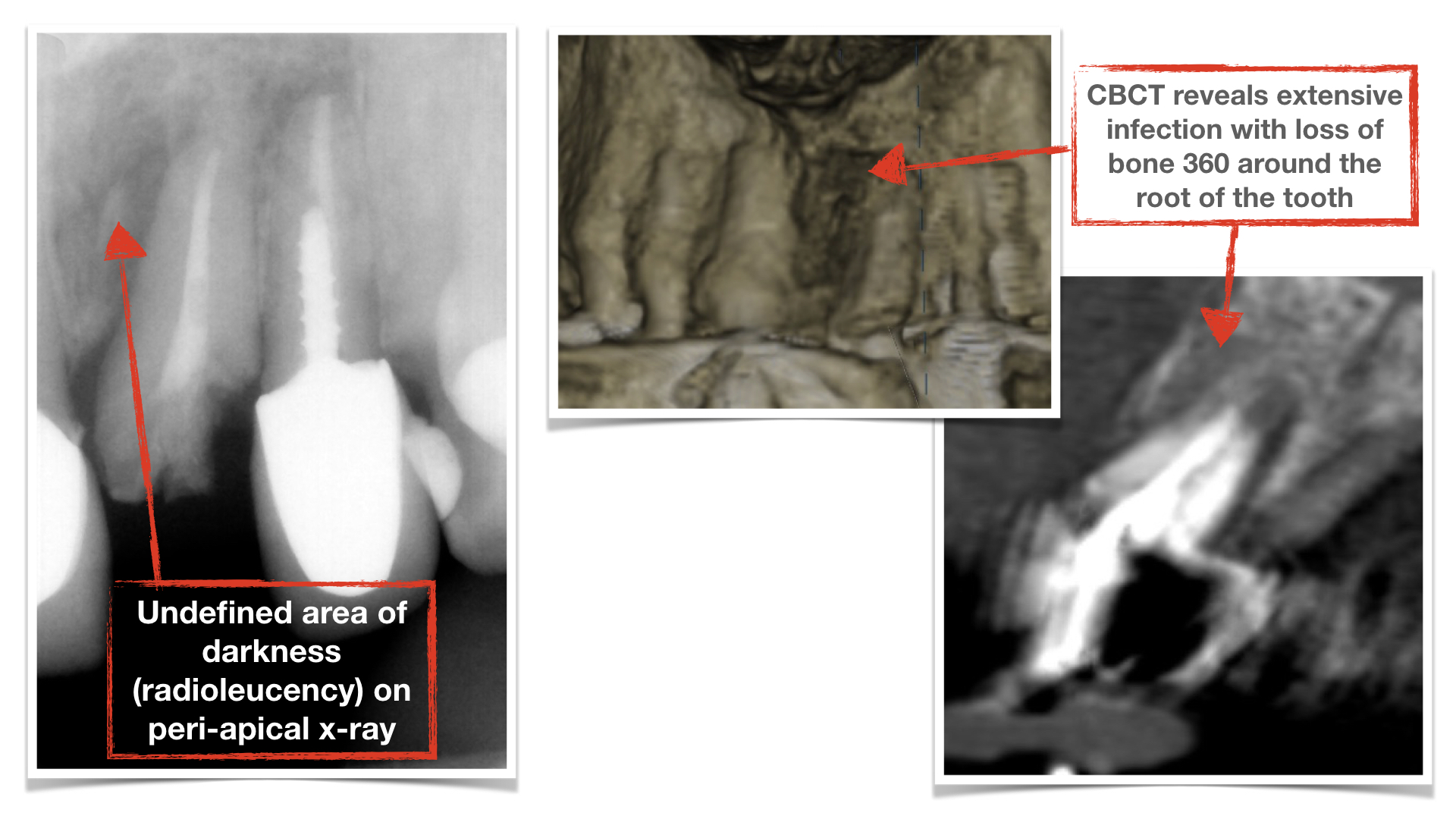
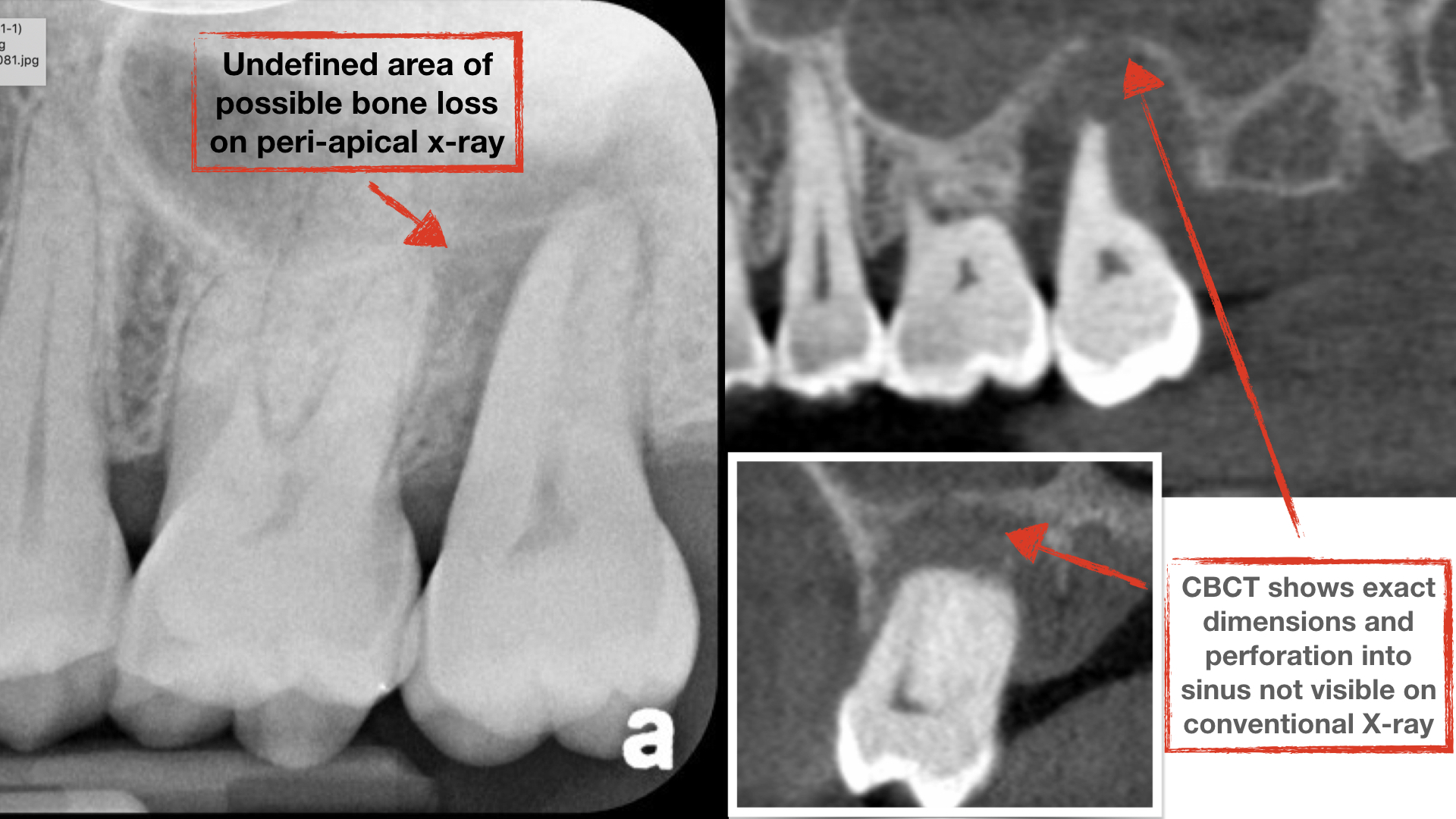
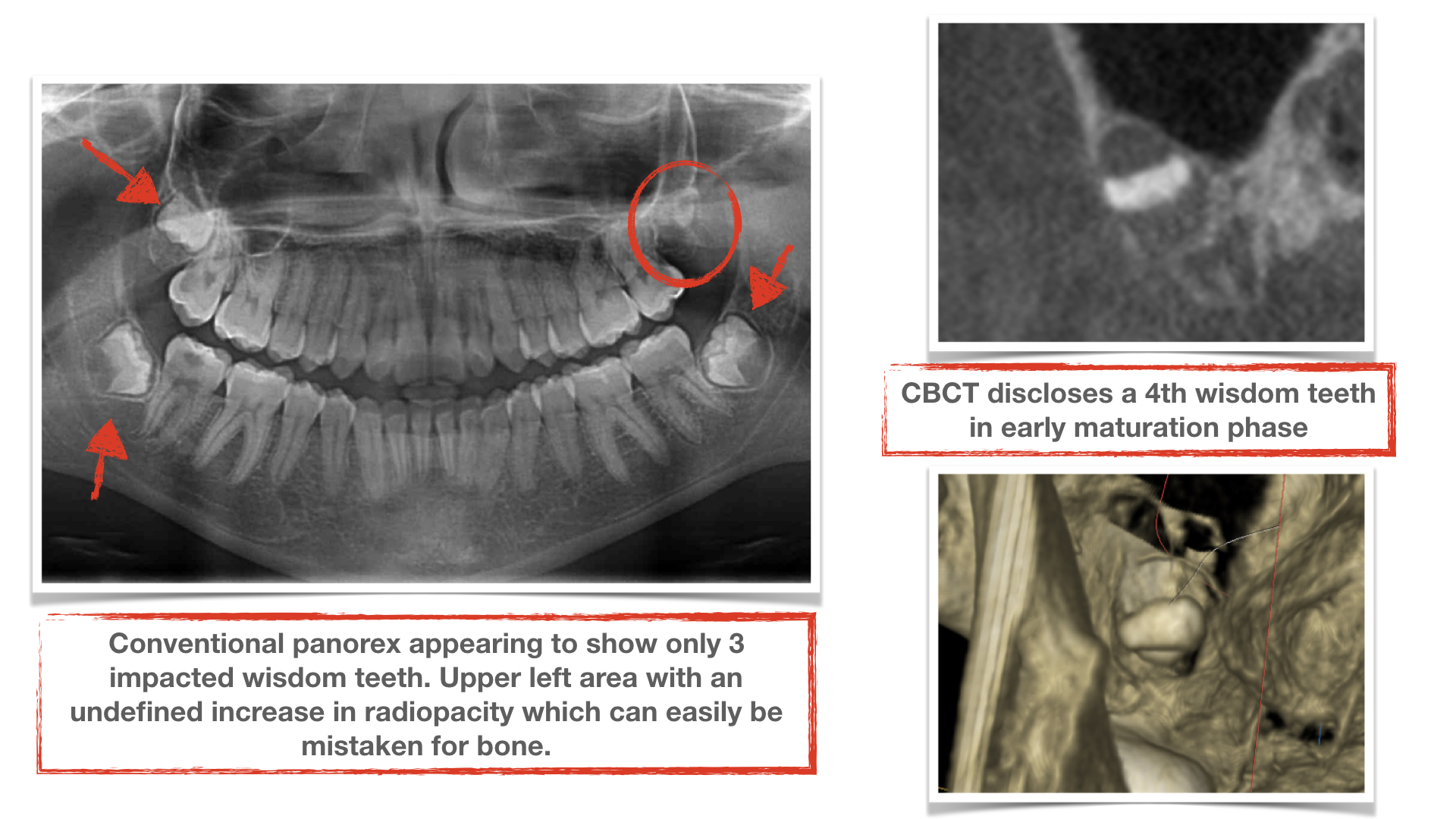
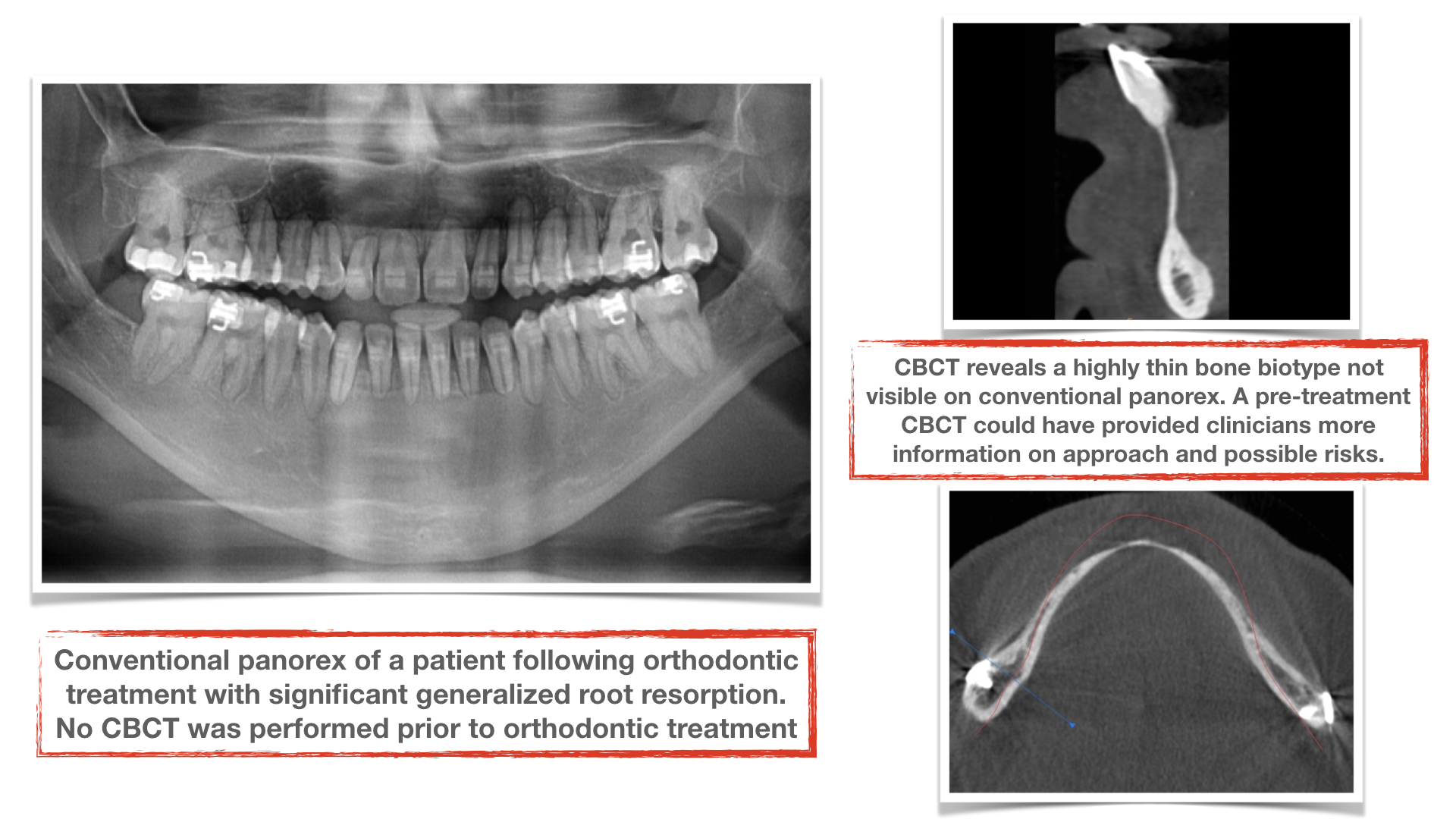
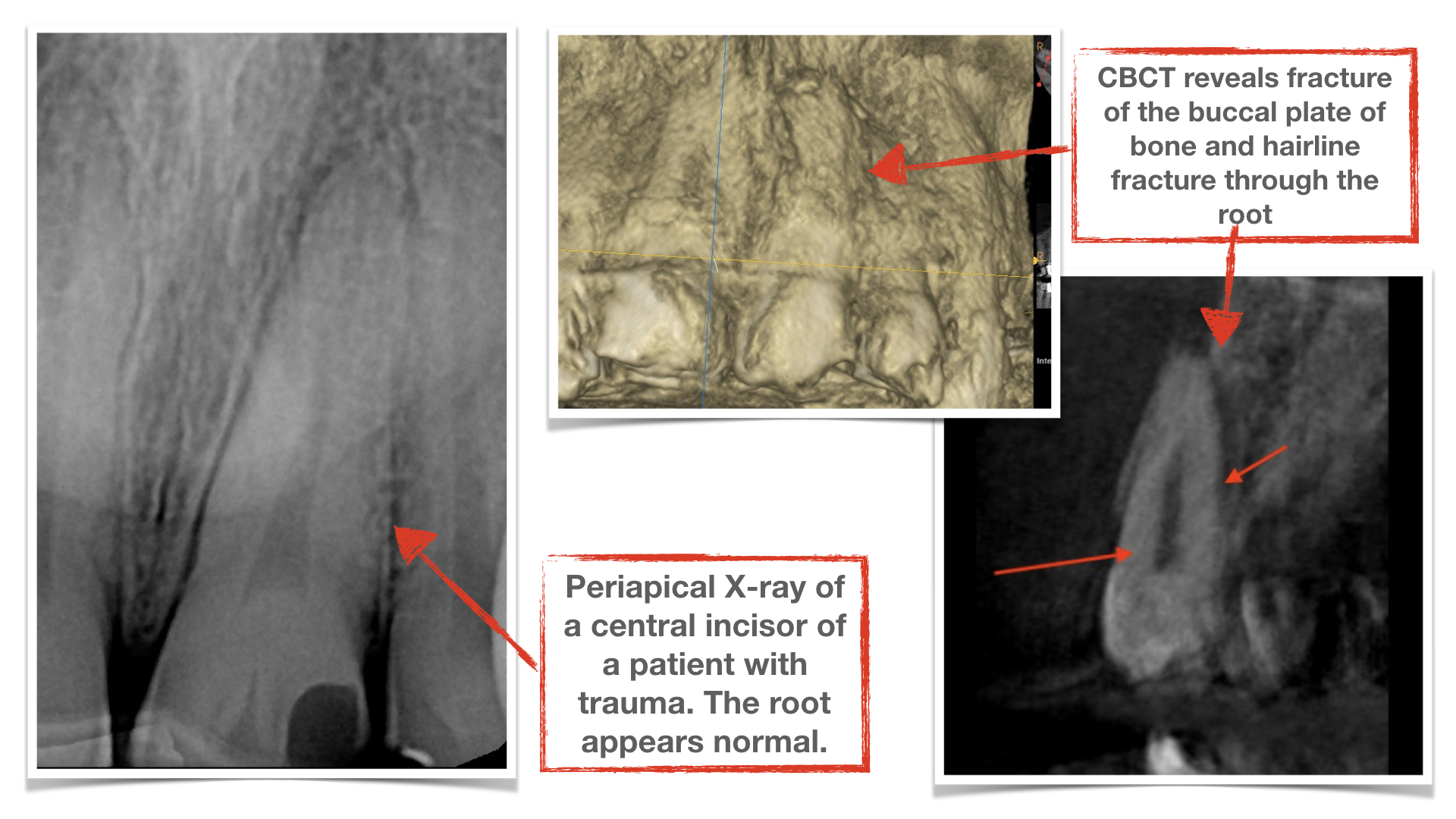
The American Dental Association put out a white paper on X-ray recommendations in 2012 and, while it provided good guidelines, it was written before the age of advanced 3-D X-ray and digital diagnostics. The recommendations included only conventional 2-dimensional X-rays such as periapical and panoramic X-rays. For many years, these were the only options. And, for many years, dentists depended on them for detection of caries, bone loss, and other abnormalities. However, it is now well recognized that such 2-dimensional X-rays do not reveal the whole picture, and many conditions can go undiagnosed or misread on such X-rays. Hence, depending solely on periapical and Panorex dental X-rays will result in incomplete diagnosis and can be detrimental, particularly in high-risk patients. Here are several examples of patients with conditions not completely detected on regular dental X-rays yet shown to have advanced destruction or deformities on a CBCT (cone beam CT scan).
[Click on image below and advance to see more:]
The ADA recommendations were clearly deficient in how and when clinicians should consider CBCT as an adjunct radiographic study in some patients. Below is an excerpt from the ADA paper on X-ray recommendations in adults:
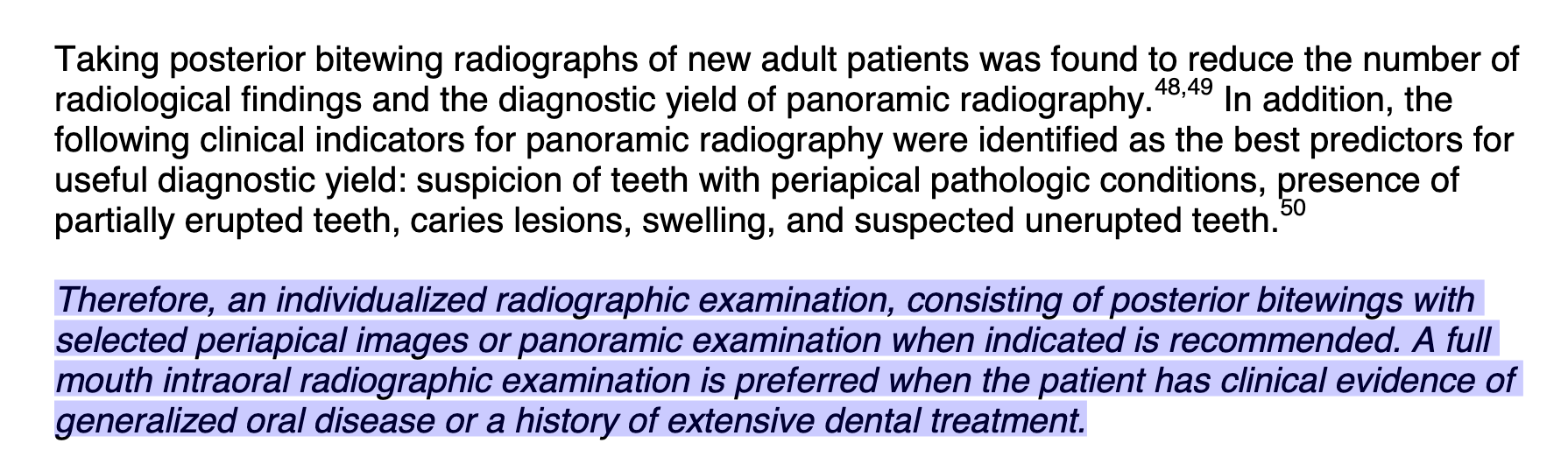
These recommendations fail to recognize that conventional X-rays are limited in their diagnostic accuracy and one cannot depend on them with 100% certainty.
Unfortunately, many in the dental profession still follow the old guidelines and continue to recommend only a Panorex and a set of bitewings for their patients’ base radiographs. At The University of Pennsylvania, where I went to dental school, as well as many other schools, students were taught to obtain as a minimum a full mouth series (FMS) of X-rays in every new patient as their baseline radiographs. Panoramic X-rays by themselves are inadequate as they are mainly diagnostic for large lesions, deformities, and general teeth positions and can have significant distortion and up to 25% magnification, making them even less accurate. They will not provide adequate diagnostic information on smaller areas of caries, defects, or abnormalities. Furthermore, bitewing X-rays are very limited in their field of view showing only the crowns of the posterior (back) teeth. Hence, Panorex and a set of bitewings by themselves are inadequate diagnostic radiographs and are not acceptable baseline X-rays for new patients.
In addition, many clinicians continue to use only 2-dimensional X-rays for sophisticated dental treatments such as dental implants, endodontics, and orthodontics. It is no surprise that the majority of complications in these patients are a direct result of poor planning and execution which are, in turn, related to inadequate imaging and diagnostic X-rays.
Recommendations for X-rays should be determined by evidence-based dentistry, patient susceptibility to dental disease, previous and current dental conditions, as well as the patient’s overall risk factors. Therefore, we suggest the following new guidelines for dental X-rays:
Adults who are new patients at a dental office (baseline X-rays):
- Full mouth series of X-rays: Consist of 14-20 small intra-oral X-rays. Full mouth series (FMS) should be the baseline X-ray for every adult patient.
- Panorex: Necessary if patient has impacted or malpositioned wisdom teeth and prior to orthodontic treatment.
- CBCT (cone beam CT scan): Necessary if patient has multiple previously treated teeth, extensive restorations, extensive history of caries, root canal treatments, periodontal disease, or is anticipating orthodontic and/or dental implant treatment. Additionally, it is indicated in patients who present with any type of bone loss related to periodontal disease, lesions of endodontic origin, or odontogenic cysts. It is also the imaging technique of choice for all types of oral and facial trauma.
Adults who are existing patients returning for regular recall visits: The frequency and type of X-rays depends on the condition of the patient’s dentition and history of treatment. There are three main categories of overall dental health:
- Overall healthy teeth with minimal caries, restorations, and healthy bone and gum tissue:
- Bitewing X-rays every 6 months
- Full mouth series of X-rays- every 2 years
- Moderate level of caries and number of restorations:
- Bitewing X-rays every 4-6 months
- Full mouth series of X-rays- every 1-2 years depending on level of disease risk (to be assessed by the treating dentist)
- Significant history of caries, restorations, multiple treated teeth either endodontically (root canals) or periodontally (gum and bone):
- Bitewing X-rays every 3-4 months
- Full mouth series of X-rays (FMS) every 6 months to 12 months
- Panoramic X-ray obtained as needed for general assessment
- CBCT- every 1-2 years depending on patient’s level of disease risk
While X-rays are of great value, we as dentists must prescribe them conscientiously and judiciously and with good rationale. We must consider the cost and exposure to radiation for every patient. We must not under- or over-utilize them but rather recommend just the right type and frequency. There are three schools of thought among dentists that we see commonly:
- Dentists who get all the X-rays (Full mouth series, Panorex, CBCT) in every patient regardless of age, disease susceptibility, or need. This is obviously excessive as the selection does not correlate to the patients’ individual needs, risk factors, and dental condition.
- Dentists who refrain from obtaining full mouth series of X-rays or CBCT either due to cost or to minimize radiation. This can put the health of patients at risk as many conditions can go undiagnosed or misread. This is not an acceptable approach as such decisions are not based on patients’ needs and clinical circumstances.
- Dentists who get the basic necessary X-rays (Full mouth series, bitewings, and Panorex as needed) and supplement with more advanced 3-D X-rays, such as CBCT, when necessary. This, in the opinion of many, is where we should be. Recommendations should be based on evidence-based dentistry and be completely patient-centered. The additional cost and radiation exposure of a full mouth series of X-rays or a CBCT are justified if they help the dentist better diagnose conditions, provide more accurate and relevant treatments, and minimize complications and patient morbidity.
What about patients who are hesitant and do not allow dentists to obtain the necessary X-rays, either as a new patient, for recall, or for specific treatments such as endodontics, orthodontics, or oral surgery? This will obviously limit the dentist’s ability to diagnose the patient’s dental condition and will prevent them from giving appropriate recommendations. In such circumstances, we must educate our patients and explain the rationale behind the recommended X-rays and help them understand the necessity. If a patient continues to decline diagnostic radiographs, the dentist will have no option but to decline treatment.
Dr. H. Ryan Kazemi is an oral and maxillofacial surgeon in Bethesda, MD.